How Your Peptide Vials
Are Created
A complete step-by-step breakdown of the freeze-drying process used to manufacture sterile, shelf-stable vials of peptides, vitamins, and other injectable compounds — and where most vendors cut corners.
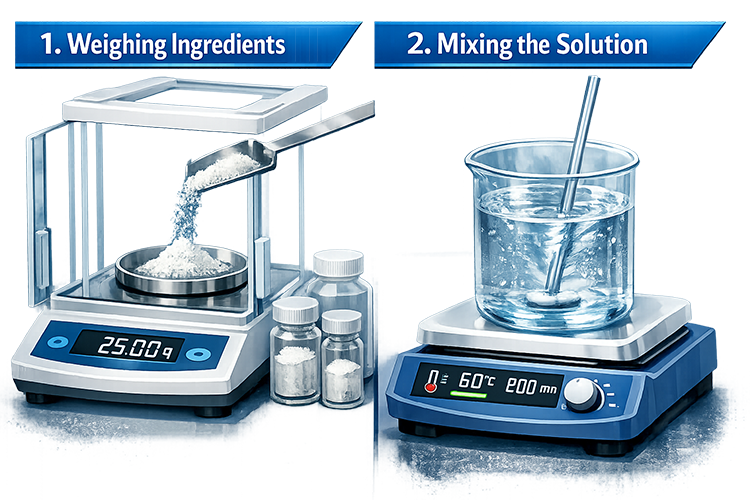
The active ingredient arrives as a raw bulk powder from a chemical or pharmaceutical supplier. Each batch should come with a Certificate of Analysis (CoA) confirming identity, purity, and absence of contaminants. The powder is precisely weighed on an analytical balance to calculate the exact amount needed for the batch based on the intended dose per vial and total vial count — accounting for dead volume losses in filters and tubing.
- No CoA review or independent raw material testing — many vendors accept supplier CoAs at face value or don't request them at all, meaning impure or mislabeled starting material goes directly into finished vials.
- Inaccurate weighing — using consumer-grade scales rather than analytical balances leads to significant dose inaccuracies, especially for potent low-dose compounds.
- No dead volume accounting — miscalculating batch size means the last vials in a batch are underfilled or underdosed.
Glass vials are not sold pre-sterile and must be processed before use. They are baked in a dry heat oven at 250°C (482°F) for 30–60 minutes. This achieves two critical goals simultaneously: sterilization (killing all microorganisms including heat-resistant spores) and depyrogenation — destroying bacterial endotoxins, which are lipopolysaccharide fragments from bacterial cell walls that survive standard steam sterilization and cause fever, inflammation, and septic shock when injected.
After baking, vials are cooled inside the oven with the door closed, then transferred directly into the laminar flow hood in a covered, clean container.
- Skipping dry heat entirely — rinsing vials with IPA or "sterile water." This is neither sterile nor depyrogenated.
- Using autoclave instead of dry heat — sterilizes but leaves endotoxins intact. Pyrogenic vials pass a basic sterility test but will still cause reactions.
- Skipping vial sterilization altogether — filling straight into off-the-shelf vials with no processing at all.

The rubber stoppers are purchased pre-sterilized and pre-siliconized from a pharmaceutical supplier — typically steam autoclaved in sealed, double-bagged packaging. Unlike glass vials, rubber cannot withstand 250°C dry heat without degrading. For stoppers, endotoxin control is handled at the supplier level, which is why sourcing from a reputable pharma-grade supplier is essential.
Stoppers are kept sealed in their original packaging and only opened inside the laminar flow hood immediately before use. Any stopper that contacts a non-sterile surface is discarded.
- Purchasing non-pharmaceutical grade stoppers — generic rubber septa from lab supply houses may not be tested for endotoxins or extractables.
- Opening stopper packaging outside the hood — even brief exposure to open air introduces contamination risk.
- Handling stoppers with bare hands — oils and microorganisms from skin are directly transferred to the sealing surface.
Every step from this point forward must be performed under a laminar flow hood (LFH) — a workstation with a HEPA-filtered, unidirectional airflow that continuously sweeps particles away from the work surface. This creates an ISO Class 5 (Class 100) environment with fewer than 100 particles ≥0.5µm per cubic foot — compared to tens of thousands in typical room air.
A vertical downflow hood is preferred for aseptic filling — air flows down from above, protecting open containers. The hood should run for 15–30 minutes before use. The operator wears nitrile gloves, a face mask, and a lab coat, and avoids movements that sweep across or upstream of open containers.
- No laminar flow hood — open bench preparation in a regular room. This is the single biggest contributor to contaminated vials and the most common shortcut taken by small gray-market operations.
- Using a still-air box as a substitute — better than nothing, but not equivalent to a true HEPA laminar flow environment.
- Not running the hood before use — particles from previous sessions or ambient air remain in the work zone.
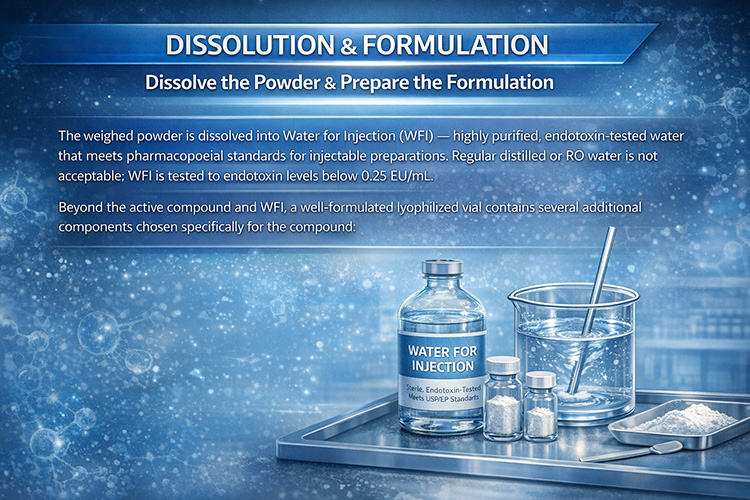
The weighed powder is dissolved into Water for Injection (WFI) — highly purified, endotoxin-tested water meeting pharmacopoeial standards for injectable preparations. Regular distilled or RO water is not acceptable; WFI is tested to endotoxin levels below 0.25 EU/mL. The solution is prepared at a concentration such that the fill volume delivers the target dose per vial.
Beyond WFI and the active compound, a properly formulated vial contains several excipient layers. The specific combination depends heavily on the compound being made. Getting this right is the difference between a vial that retains potency for 12–24 months and one that degrades within weeks.
── Layer 1: Bulking Agent / Cryoprotectant ──
Mannitol is the most common. It crystallizes during lyophilization, producing a clean, firm, elegant white cake with excellent structural integrity. Ideal for simple peptides and vitamins.
Trehalose remains amorphous (glassy) during lyophilization. This glassy matrix forms a protective shell directly around each molecule, preserving tertiary structure and conjugation sites. Strongly preferred for complex peptides, proteins, and fatty-acid conjugated compounds (GLP-1 agonists).
Sucrose behaves similarly to trehalose and is used interchangeably in many formulations. Some formulations combine mannitol + trehalose to get both structural integrity and molecular protection.
── Layer 2: Buffer & pH ──
Most compounds have a pH window where they are most stable. Sodium phosphate (pH 6.0–7.5) is the most common general-purpose buffer. Sodium citrate (pH 3.0–6.5) is preferred for acidic-stability compounds like NAD+. Histidine (pH 5.5–7.0) is the preferred buffer for GLP-1 agonists (semaglutide, tirzepatide, retatrutide) — it also has mild antioxidant and metal-chelating properties.
── Layer 3: Surfactant (Aggregation Prevention) ──
Polysorbate 80 (Tween 80) at 0.01–0.05% is the standard choice for GLP-1 agonists — used in the commercial semaglutide formulation. It prevents the peptide from aggregating at surfaces. Polysorbate 20 is used for smaller, less hydrophobic peptides.
── Layer 4: Antioxidant Stabilizers ──
Free methionine amino acid (1–10mM) acts as a sacrificial antioxidant — any oxidizing species in the vial preferentially attacks the free methionine rather than the methionine residue in the peptide backbone. Ascorbic acid is a direct antioxidant scavenger. EDTA at 0.01–0.1mg/mL is a metal chelator that removes trace metal contamination which catalyzes oxidation reactions.
── Compound-Specific Formulation Reference ──
| Compound | Cryoprotectant | Buffer / pH Target | Antioxidant | Chelator | Surfactant | N₂ Headspace |
|---|---|---|---|---|---|---|
| B12 (Cyanocobalamin) | Mannitol | Phosphate / pH 6.0–7.0 | Not needed | Not needed | Not needed | Amber vial only |
| BPC-157 | Mannitol | Phosphate / pH 6.5–7.0 | Not needed | Not needed | Optional PS80 | Not critical |
| Ipamorelin / CJC-1295 | Mannitol | Phosphate / pH 6.5–7.0 | Not needed | Not needed | Optional PS80 | Not critical |
| TB-500 (Thymosin β4) | Mannitol or Trehalose | Phosphate / pH 6.5–7.0 | Free Met (contains Met) | Optional EDTA | PS80 | Recommended |
| Selank / Semax | Mannitol | Phosphate / pH 6.5–7.0 | Not needed | Not needed | Optional PS20 | Not critical |
| AOD-9604 / HGH Frag | Mannitol | Phosphate / pH 6.5–7.0 | Not needed | Not needed | Optional PS80 | Not critical |
| Tesamorelin | Mannitol + Trehalose | Phosphate / pH 6.5–7.0 | Free Met | EDTA | PS80 | Recommended |
| Semaglutide | Trehalose (required) | Histidine / pH 6.0–6.5 | Free Met (contains Met) | EDTA | PS80 (required) | Important |
| Tirzepatide / Retatrutide | Trehalose (required) | Histidine / pH 6.0–6.5 | Free Met + Ascorbic acid | EDTA | PS80 (required) | Important |
| NAD+ | Trehalose | Citrate / pH 5.0–6.0 | Ascorbic acid | EDTA | Not needed | Critical |
| Epithalon / Short Peptides | Mannitol | Phosphate / pH 6.5–7.0 | Not needed | Not needed | Not needed | Not critical |
- Using regular distilled or RO water instead of WFI — endotoxin levels are uncontrolled, creating pyrogenic risk in every vial regardless of how well everything else is done.
- No pH adjustment or buffering whatsoever — the single most common shortcut. The compound is simply dissolved in plain water and filled.
- Mannitol only, regardless of compound — for semaglutide, tirzepatide, and retatrutide, mannitol's crystallization during lyophilization can exclude the peptide from the protective matrix entirely.
- No surfactant for GLP-1 agonists — without Polysorbate 80, fatty-acid conjugated peptides aggregate during freezing and reconstitution. The aggregated fraction is biologically inactive.
- No free methionine or EDTA for Met-containing peptides — oxidation of the methionine residue changes the peptide's conformation and reduces or eliminates activity.
- This entire formulation layer is typically skipped entirely by Chinese gray-market suppliers — most source peptide powder, dissolve it in plain water with mannitol, filter, fill, and freeze dry. No pH measurement, no buffer, no surfactant, no antioxidants, no chelator.
The prepared solution is passed through a 0.22 micron sterile PES membrane filter — a syringe filter for small batches, or an inline capsule filter for larger volumes. This is the final bioburden reduction step, removing all bacteria and fungal spores. The filter is single-use and discarded after the batch. Filtration is performed directly into the sterile fill vessel inside the laminar flow hood.
Note: 0.22µm filtration does not remove viruses or endotoxins — which is why starting material quality, WFI, and vial depyrogenation all matter independently.
- Skipping sterile filtration entirely — filling directly from the mixed solution. Any contamination introduced during mixing goes into every vial.
- Reusing filters across batches — a used filter becomes a contamination source and may lose membrane integrity.
- Using the wrong filter material — proteins and some peptides bind to nylon membranes, causing significant active compound losses. PES (polyethersulfone) is low-binding and the correct choice.

Using a calibrated syringe, repeating pipette, or volumetric fill pump, each vial receives an exact, consistent volume of solution. Dose accuracy is achieved through volume control — not weighing — because the solution concentration is already precisely known. A consistent fill volume guarantees a consistent dose. All filling is performed inside the laminar flow hood with vials never left open longer than necessary.
Vial Sizing & Fill Volume: Fill volume isn't just about dose — it also determines cake geometry and drying performance. As a general rule, the fill should occupy no more than 30–40% of the total vial volume. A 10mL vial, for example, should receive no more than 3–4mL of solution. Fill depth also matters: shallower fills dry faster and more uniformly. Too little fill in an oversized vial produces a thin, fragile disc that customers may mistake for an underdosed or empty vial.
- Uncalibrated or consumer-grade syringes — 5–15% fill volume variation between vials is common, leading to significant dose inconsistency across a batch.
- Filling outside the laminar flow hood — open vials on an unprotected bench during the most contamination-vulnerable step in the process.
- Rushing the fill — too fast introduces air bubbles, splashing, and volume errors.
- Mismatched vial size and fill volume — using whatever vials are on hand rather than selecting the right size for the fill.

A rubber stopper is placed into the opening of each filled vial but left partially seated — resting at a partially inserted position that allows water vapor to escape during freeze-drying while still protecting the opening from gross contamination. A fully seated stopper would trap water vapor and prevent the product from drying properly. Vials are transferred to the freeze dryer trays immediately after stoppering.
- Fully seating stoppers before lyophilization — traps moisture, resulting in high residual water content in the final product despite appearing dry.
- Long delays between filling and loading the freeze dryer — partially stoppered vials sitting on a bench for hours dramatically increase contamination risk.

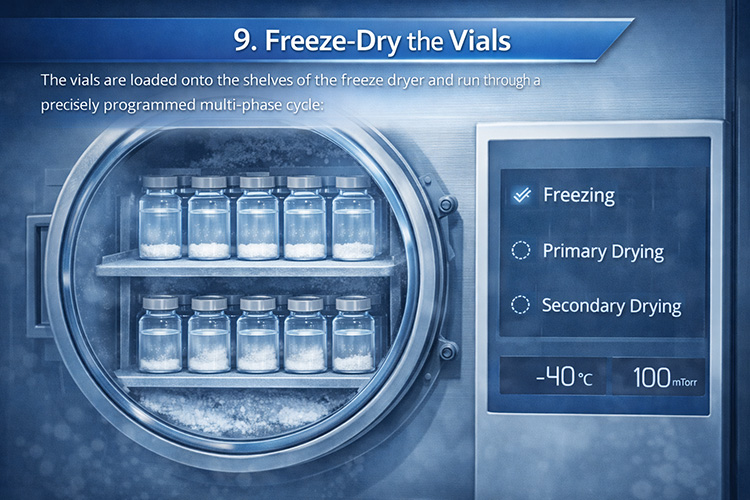
The vials are loaded onto the shelves of the freeze dryer and run through a precisely programmed multi-phase cycle:
1. Freezing — shelf temperature drops to –40°C to –50°C, solidifying the liquid completely. Freezing rate affects ice crystal size, which impacts drying speed and product quality.
2. Primary Drying (Sublimation) — chamber is evacuated to deep vacuum (100–200 mTorr) and shelf temperature rises slightly (–20°C to –10°C). Ice sublimates directly to vapor, which is captured by a cold condenser at –60°C to –80°C. This removes ~90–95% of the water and takes 12–24+ hours depending on fill volume.
3. Secondary Drying (Desorption) — shelf temperature increases further (+20°C to +40°C) to remove residual bound moisture, bringing residual water below 1–2%. Cutting this phase short is a common cause of premature product degradation.
The result is a porous, dry "cake" — a white, solid matrix that reconstitutes quickly when bacteriostatic water is added back.
- Unvalidated lyophilization cycles — guessing at time and temperature rather than developing a proper cycle for each specific formulation and fill volume.
- Cutting secondary drying short — to save time. The product looks dry but residual moisture is high, dramatically shortening shelf life.
- Overloading the freeze dryer — too many vials for the condenser capacity results in uneven drying across the batch.
- Overfilled vials relative to vial size — a fill that's too deep for the vial diameter creates an uneven drying front, often resulting in a partially collapsed or unevenly dried cake that looks normal from the outside but has elevated residual moisture.
For compounds susceptible to oxidative degradation — NAD+, peptides with methionine or cysteine residues, and other redox-active molecules — oxygen in the vial headspace will slowly degrade the product over time even in the dry state.
The proper method uses a freeze dryer with a nitrogen inlet port: at the end of secondary drying, instead of venting the chamber with air, the chamber is backfilled with filtered dry nitrogen (or argon) before the stoppers seat. The vial headspace is then nitrogen — no oxygen present.
Smaller operations without this capability can alternatively flow nitrogen gently over the vials immediately before stopper insertion. This is a compromise but meaningfully better than air-filled headspace for sensitive compounds.
- Air headspace in all vials regardless of compound — most small operations don't have nitrogen inerting capability or don't know it's relevant. For NAD+ and similar compounds, this significantly shortens shelf life.
- No antioxidant excipients in the formulation either — the combination of air headspace and no antioxidant stabilizers means oxidation-sensitive products degrade well before their labeled expiry.
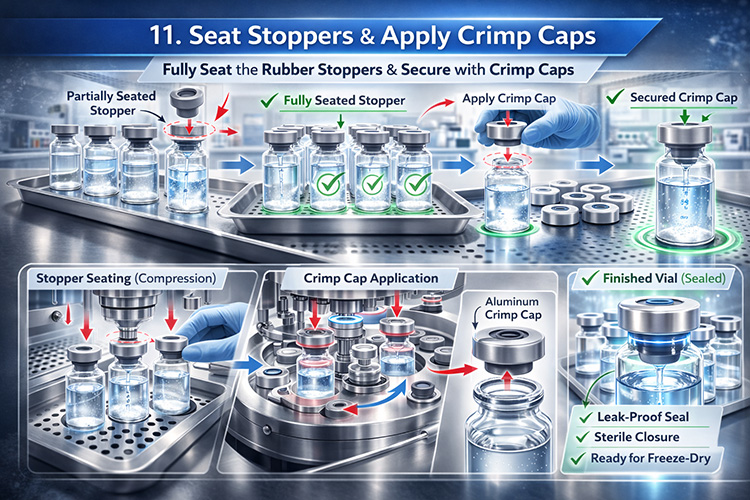
When the freeze dryer cycle completes and the chamber is vented, atmospheric pressure outside the vial immediately holds the partially-seated stopper firmly in place — the vacuum inside acts exactly like a canned jar lid held down by atmospheric pressure differential. The stoppers are then fully pressed home and an aluminum crimp cap is applied over the stopper using a hand crimper or benchtop crimping tool.
The crimp cap mechanically locks the stopper and provides tamper evidence — it is not what maintains the vacuum or sterility. The stopper and internal vacuum do the actual sealing work. Labels including compound name, lot number, dose, and reconstitution instructions are applied.
- Opening the freeze dryer door fully before venting completely — a rush of unfiltered room air into the chamber before stoppers are seated can deposit particulates directly into vials.
- Missing or incomplete labels — no reconstitution instructions, no concentration, no lot number, no expiry. The end user cannot verify what they have or use it safely.
Every finished vial should be individually inspected against a light box or bright lamp against a dark background:
Particulates: visible particles in the cake or on vial walls — indicates contamination or aggregation.
Cake appearance: a good cake is white, uniform, intact, and fills most of the vial. A collapsed cake (sunken, shrunken, sticky residue) means primary drying temperature was too high and the product may be damaged. Browning indicates thermal degradation.
Stopper seating: all stoppers fully seated, none partially out.
Vial integrity: no cracks or chips. Failed vials should be quarantined — they signal a process problem that needs investigation, not just individual rejection.
- No visual inspection — all vials shipped regardless — collapsed cakes, particulates, and improperly seated stoppers all reach the customer.
- No finished product testing — no third-party HPLC potency check, no sterility test, no endotoxin test. The vendor has no idea whether what they made matches the label.
Lyophilized does not mean indestructible or room-temperature stable. Most lyophilized peptides and supplements should be stored at 2–8°C (refrigerated) for short-to-medium term, or –20°C (frozen) for long-term storage. Light-sensitive compounds should be in amber vials or foil pouches.
An underappreciated problem is freeze-thaw cycling — even though the product is dry, repeated temperature fluctuations from frequently opening a freezer door cause micro-condensation and mechanical stress on the cake matrix. Over time this degrades product quality even without ever reconstituting the vial.
A practical solution is storing vials in an insulated container such as a Hydrapeak or similar vacuum-insulated vessel kept inside the freezer. The thermal mass buffers against the temperature spike every time the freezer is opened. Store vials upright — never on their side.
- Shipping without cold packs or insulation — vials spend days at ambient temperature in transit, significantly degrading heat-sensitive products before they reach the customer.
- No storage guidance provided to customers — customers store vials at room temperature or in poorly managed freezers, not knowing this affects product quality.
- Clear vials for light-sensitive compounds — NAD+ and several peptides are photo-sensitive; clear glass offers zero UV protection.
Vendor Quality Scorecard
Use this as a framework to evaluate any lyophilized product source. Quality vendors are transparent about their process; poor ones aren't.
- No CoA available for raw materials or finished product
- No third-party HPLC or potency testing published
- Collapsed, brown, or inconsistent cake appearance
- No reconstitution instructions on label
- Visible particulates after reconstitution
- Ships without cold packs
- No lot numbers or expiry dates
- Claims room-temperature stability for heat-sensitive compounds
- Won't describe their manufacturing environment
- Sterility or endotoxin test failures in independent testing
- Third-party HPLC potency results published per lot
- Sterility and endotoxin testing on finished product
- Clean white intact cake, consistent across vials
- Clear labeling: compound, dose, lot, expiry, reconstitution volume
- WFI used, formulation includes appropriate excipients
- Nitrogen inerting for oxidation-sensitive products (NAD+, etc.)
- Cold chain shipping with temperature monitoring
- Documented batch records and process transparency
- Validated lyophilization cycles per compound
- Amber vials for light-sensitive compounds
Understanding Lab Test Results & Vendor Discrepancies
Third-party HPLC testing from labs like Janoshik or Finnrick is the community standard for verifying gray market peptide products. But the results are widely misread. Understanding what those numbers actually mean — and what they don't — changes how you evaluate vendors entirely.
- Identity — Is this actually retatrutide and not something else? High confidence.
- Purity — What percentage of the sample is the target compound vs impurities? High confidence.
- Presence of contaminants — Are there unexpected peaks indicating degradation products or adulterants? High confidence.
- Absolute mg content per vial — The number that looks most important is actually the least reliable. A result of 58mg on a 60mg vial is within measurement noise, not evidence of underdosing.
- What the patient actually receives — Testing a single vial says nothing about batch consistency.
When a lab reports 58mg on a 60mg vial, that number carries accumulated uncertainty from two independent sources — the vendor's manufacturing process and the lab's own measurement. Stack them together and the real uncertainty is far wider than the single decimal point suggests.
- Uncalibrated fill equipment: ±5–10%
- Raw material weighing: ±2–3%
- Filter and dead volume losses: ±3–5%
- Vial-to-vial fill variation: ±3–5%
- Lyophilization losses: ±2–3%
- Reconstitution completeness: ±3–5%
- Sample prep pipetting: ±2–3%
- Reference standard uncertainty: ±5–10%
- Instrument calibration: ±1–2%
- Extinction coefficient assumptions: ±5–10%
Combined realistic uncertainty: ±15–25% on absolute mg content. A 60mg vial could genuinely contain anywhere from 45–75mg and still produce a test result of 58mg at a competent lab. The number looks precise. It isn't.
For approved drugs like semaglutide and tirzepatide, certified reference standards exist. For retatrutide, which remains in clinical trials, a certified reference standard may not be commercially available. Without it, labs estimate quantity using UV absorbance at 214nm with a generic peptide extinction coefficient. The actual extinction coefficient varies by peptide sequence and can differ 10–20% from the generic assumption — introducing a systematic bias that shifts every result in the same direction without ever appearing as scatter or noise.
- The compound is what it claims to be — high confidence. This is genuinely valuable.
- Purity is approximately as stated — high confidence. Major impurities or adulterants will show up.
- The dose is in the right ballpark — moderate confidence. Is it 60mg or actually 20mg? That you can tell. Whether it's 58mg vs 62mg you cannot.
- Nothing about batch consistency — a single vial tells you nothing about the other 99 vials in the batch.
Forum posts debating whether 56mg vs 60mg means a vendor is underdosing are treating measurement noise as meaningful signal. A 4mg difference on a 60mg vial is a 6.7% deviation — well within the combined measurement uncertainty of any lab working with unapproved compounds.
What would actually indicate a real problem: results consistently clustering at 40–45mg across multiple vials from the same batch, or a result of 30mg on a labeled 60mg vial. A pattern across multiple tests tells you something. A single result within 10% of label claim tells you almost nothing about dosing accuracy — only that the compound is present and approximately correct.
When you make your own vials with a calibrated analytical balance (0.1mg resolution), a calibrated repeating syringe, a precisely prepared solution of known concentration, and consistent fill volumes — your actual dose accuracy will be better than ±5% vial-to-vial. This is tighter than any gray market vendor operating without calibrated equipment, and tighter than what any lab can actually verify from a finished vial. The math and the process are working in your favor. You know your solution concentration. You know your fill volume. The dose is the product of those two numbers and both are under your control.